Sacrocolpoplexy
What is a sacrocolpopexy?
A sacrocolpopexy is a surgical procedure used to treat pelvic organ prolapse. Pelvic organ prolapse is a condition that is caused by a weakening of the normal support of the pelvic floor, and is similar to a hernia in the vagina.
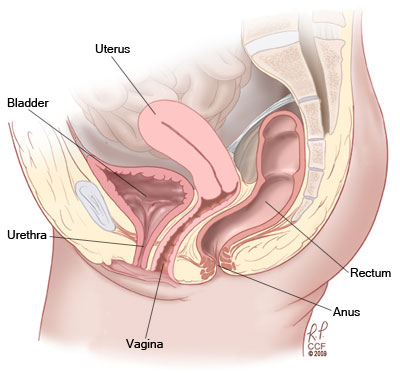
The organs of the pelvis—the area of the body between the hip bones—include the vagina, uterus, cervix, bladder, urethra (the tube through which urine passes), intestines and rectum. These organs are held in place by a group of muscles and other support tissue. When this support system becomes stretched, weakened, or torn, it allows pelvic organs to slip out of their normal places or sag down (prolapse).
There are different types of prolapse, depending on the organ or organs involved. These include:
- Uterine prolapse: The uterus and cervix drop down the vaginal canal, sometimes so far that they go past the vaginal opening.
- Vaginal vault prolapse: The top of the vagina (known as the “vaginal vault”) drops down the vaginal canal. This occurs in women who have previously had a hysterectomy (removal of the uterus).
- Cystocele: The bladder bulges into the vagina.
- Rectocele: The rectum bulges into the vagina.
- Enterocele: The small intestine bulges against the vaginal wall. An enterocele and vaginal vault prolapse can occur together.
What causes pelvic organ prolapse?
The most common causes of pelvic organ prolapse are the following:
- Childbirth: Vaginal delivery increases the risk of prolapse more than a cesarean section (when the baby is delivered through a surgical opening in the wall of the abdomen).
- Surgery, such as a hysterectomy
- Aging
- Extreme physical activity or lifting of heavy objects
- Any condition that is associated with increased abdominal pressure, such as being overweight, frequently straining to have bowel movements, or having a chronic cough
- Genetic (hereditary) factors: One person’s pelvic support system may be naturally weaker than another’s.
Procedure Details
How is prolapse repaired with a sacrocolpopexy?
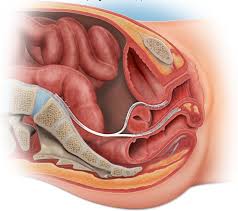
In a sacrocolpopexy procedure, the surgeon attaches surgical mesh from the vagina to the sacrum (tail bone), which is the bone at the base of the spine. If a patient still has her uterus, the surgeon may decide to remove it, with or without leaving the cervix in place. If the cervix is left in place, the mesh will be applied over the top of the cervix, as well as to the vaginal walls.
A sacrocolpopexy is usually performed laparoscopically (through small incisions, or cuts) in the following way:
- General anesthesia is administered so that the patient is asleep during the procedure.
- Four to five incisions are made on the abdomen.
- The abdomen is inflated with carbon dioxide gas to create space to perform the surgery.
- A laparoscope (a thin, telescope-type tube with a camera) and other instruments are passed through the incisions.
- A piece of surgical mesh is attached to the front and back walls of the vagina and then to the sacrum to suspend the top of the vagina or the cervix back into its normal position.
- In many cases, the surgeon will also remove the uterus, but may leave the cervix in place if it is still present. Some women also choose to have their Fallopian tubes and/or ovaries removed, depending upon age and family history.
- If there is not enough support for the bladder or rectum, the surgeon may repair these areas, usually through the vagina.
- If the patient has urinary incontinence, the surgeon may place a small piece of mesh underneath the urethra to give support when the patient coughs, laughs or sneezes.
- At the end of the surgery, a small camera is used to examine the inside of the bladder to ensure there were no injuries during the surgery.
The surgery takes 2-3 hours to complete. When it is over, the patient will be taken to the Post-Anesthesia Care Unit (PACU) to wake up from anesthesia.
What happens after a sacrocolpopexy?
A patient will stay in the PACU until the anesthesia wears off. If the caregivers have any concerns about the surgery, the patient may need to stay in the hospital overnight for observation.
A voiding trial will be performed to see if the catheter in the bladder can be removed before the patient is discharged home. The bladder will be filled with saline (salt water) and the catheter will be removed. If the patient is able to void (pass, or urinate) 2/3 of the volume placed in the bladder, then she will be discharged without a catheter.
If she is unable to empty her bladder completely, the catheter will be replaced and a nurse will teach her how to care for it. A follow-up appointment will be scheduled in 3-5 days for another voiding trial.
What should the patient do after a sacrocolpopexy?
The patient will have 3-5 incisions on her abdomen, which will be closed with either glue or tape. She should keep the incisions clean, dry and open to the air. The stitches that are placed underneath the skin will dissolve on their own and do not need to be removed.
The patient should wash her hands often, especially before touching her incisions, changing any dressings, after using the restroom and before eating.
Other suggestions to help with recovery:
- The patient should get plenty of rest after the procedure. A responsible adult should stay at home the first one or two nights after surgery.
- Side effects from the anesthesia can include sleepiness and confusion, which can last up to 24 hours after surgery.
- The patient may have gas pain, abdominal swelling, or shoulder pain for 24 to 72 hours after surgery because of the gas used to inflate the abdomen. A warm shower, heating pad, and/or walking may help with any discomfort.
- For the first 24 hours, the patient should take ibuprofen every 6 hours and the narcotic medication as needed. After the first day of surgery, she can take the ibuprofen as needed for pain.
- The narcotic pain medications can sometimes cause constipation. The patient will be given a prescription for medications to help reduce the chances of becoming constipated.
- At home, she should drink plenty of fluids and initially eat bland, low-fat foods such as crackers, Jell-O and chicken broth. She should try to avoid fatty foods, which can cause nausea, and then gradually expand her diet, as tolerated.
- The patient should walk gently around the house to exercise her calf muscles and prevent blood clots from developing in her legs.
- To prevent the lungs from becoming infected, the patient will be provided with a breathing machine called an incentive spirometer. She should use this device every hour to take deep breaths for the first several days after her surgery.
- If the patient is discharged home with a catheter, she should: be sure to empty the bag before it gets too full; keep the catheter tubing free of kinks; keep the Foley bag below the level of the bladder; and, keep her pubic area and catheter tubing clean.
- It is normal to have some drainage or a small amount of bleeding from the vagina after surgery. This may last up to 6 weeks.
- Recovery from surgery usually takes two to four weeks, but sometimes longer if more strenuous activity is planned. It is normal to be very tired during this time.
- A patient may shower 48 hours after the surgery, but she should NOT swim or soak in water for 6 weeks after surgery.
- The patient should go slowly on stairs and use the railing, especially the first day after surgery.
The patient should NOT:
- Do any vacuuming or push any heavy doors or grocery carts.
- Do any heavy lifting, pushing, or pulling, for 4-6 weeks.
- Lift anything more than 5 pounds, such as laundry, groceries, children, or pets.
- Put anything in the vagina for 6 weeks after surgery unless the doctor tells her to. This includes tampons, douching and sexual intercourse.
- Drive for 2 weeks after surgery, while narcotic pain medication is being taken, or until the she feels that she is ready.
When to Call the Doctor
When should a patient call her doctor after a sacrocolpopexy?
A patient should call her doctor if any of the following happen:
- She cannot urinate for 3 to 5 hours, or can only urinate small amounts.
- She develops a temperature of more than 100.4°F or 38.0°C or chills.
- She has problems with her incisions, such as redness, warmth, swelling or foul-smelling drainage.
- She develops severe nausea or persistent vomiting.
- She has bright red vaginal bleeding and is soaking more than one pad an hour.
- She has foul-smelling vaginal drainage.
- She has severe pain that does not get better when she is taking the pain medications she was provided.
- She has pain and swelling in her legs, especially if it is only on one side.
- If urination becomes painful, or if the urine becomes cloudy or foul-smelling.
References:
- National Association for Continence. Pelvic Organ Prolapse (https://www.nafc.org/pelvic-organ-prolapse/). Accessed 12/19/2018.
- American College of Obstetricians and Gynecologists. Surgery for Pelvic Organ Prolapse (https://www.acog.org/Patients/FAQs/Surgery-for-Pelvic-Organ-Prolapse). Accessed 12/19/2018.
- U.S. Department of Health and Human Services. Office on Women’s Health. Pelvic organ prolapse (https://www.womenshealth.gov/a-z-topics/pelvic-organ-prolapse). Accessed 12/19/2018.
- U.S. Food and Drug Administration. Urogynecologic Surgical Mesh Implants (https://www.fda.gov/medical-devices/implants-and-prosthetics/urogynecologic-surgical-mesh-implants). Accessed 12/19/2018.