Sterilization
Sterilization
Tubal Ligation - Female Sterilization
Introduction
Tubal ligation is usually a permanent form of birth control. It is a female sterilization procedure commonly referred to as “tying the tubes.” It is not recommended as a temporary or reversible form of birth control, and should only be used by women that are certain they do not want to have children. Tubal ligation is usually an outpatient surgery with a short recovery time.
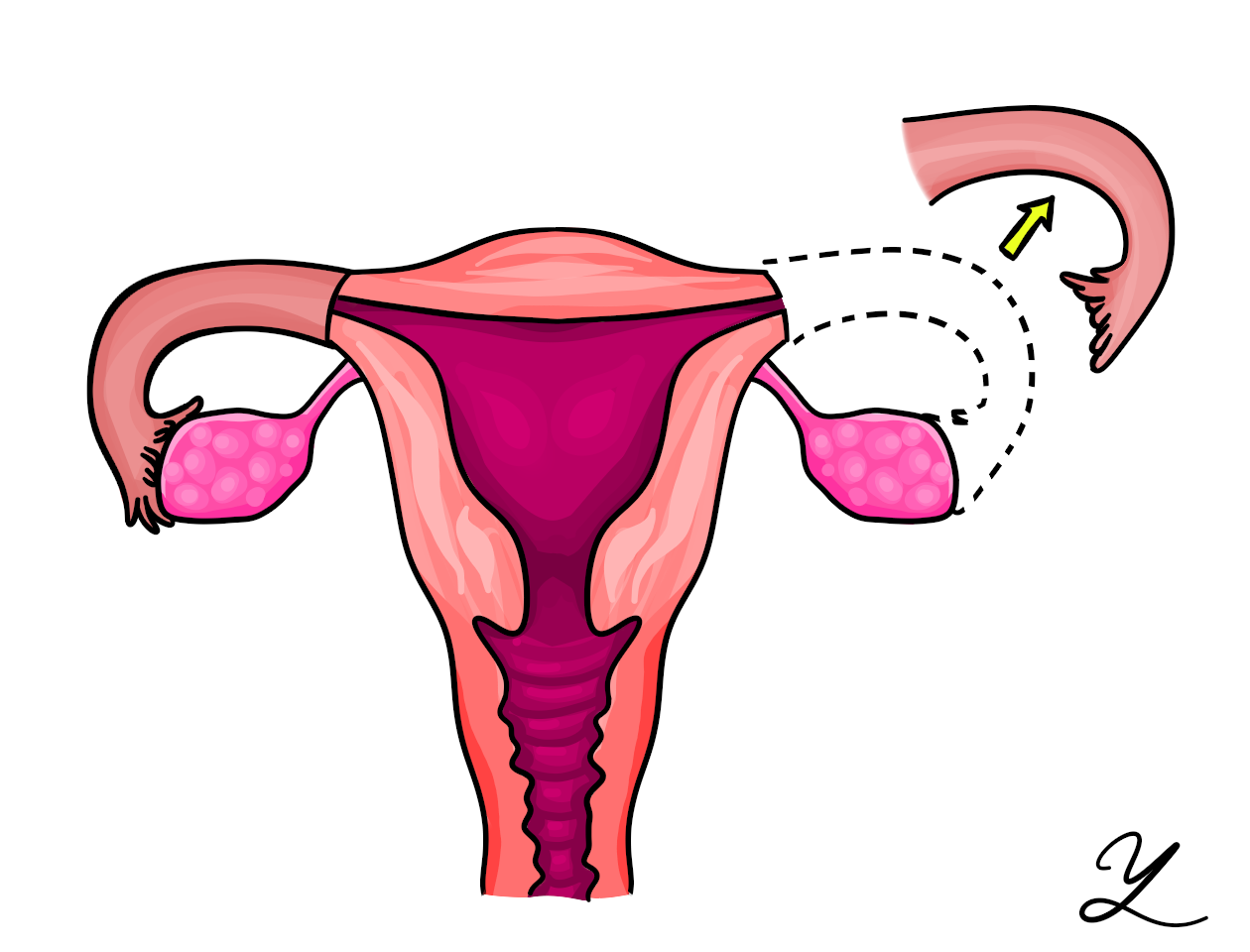
The internal female reproductive system includes the ovaries, fallopian tubes, uterus, cervix, and vagina. The ovaries are two small organs that produce eggs (ova) and hormones. An ovary typically releases one mature egg each month. Two fallopian tubes extend from near the ovaries to the uterus. The fallopian tubes transport the mature eggs to the uterus. A tubal ligation interrupts the fallopian tubes so that an egg does not have contact with sperm, and pregnancy cannot occur. You will still ovulate following tubal ligation, but the eggs will be absorbed by your body instead of traveling through the fallopian tubes and into the uterus.
Treatment
Tubal ligation is usually an outpatient procedure that may be performed at a hospital or outpatient surgery center. You will be sedated with general anesthesia and will need to have someone else drive you home following your surgery. Tubal ligation can also be done immediately following a cesarean section or vaginal childbirth.
Your surgeon will make a few small incisions in your belly button area. A laparoscope is used for the procedure. A laparoscope is a type of endoscope. It consists of a thin tube with a light and viewing instrument. Images from the laparoscope may be sent to a video monitor to guide the surgeon during the surgery. Thin surgical instruments are sent through the laparoscope and the fallopian tubes are closed with a clip or cauterized. Cauterization uses heat to burn the fallopian tubes to cause scar tissue to close them. When your procedure is complete, your incisions are closed with a few stitches.
Your doctor will recommend or prescribe pain medication to relieve discomfort following your procedure. Your doctor will provide you with specific instructions, but typically women are advised to avoid strenuous exercising for several days. Most women return to work within a few days. You will have a follow-up appointment to have your stitches removed.
Sterilization procedures can provide permanent birth control to women who no longer wish to become pregnant. Several options are available, including minimally invasive techniques. They all have the effect of blocking the Fallopian tubes so that sperm and egg cannot meet and, therefore, fertilization cannot occur. In tubal ligation, popularly called “having one’s tubes tied,” the Fallopian tubes are clamped shut with a clip or ring or are sealed shut using electrical energy. In tubal occlusion, the Fallopian tubes are blocked with small implants that encourage the growth of scar tissue, ultimately sealing off the tubes. No form of sterilization provides protection against sexually transmitted diseases.
Laparoscopic sterilization is the procedure most commonly used for tubal ligation. A small incision is made under the navel for insertion of a laparoscope – a thin, telescope-like device with a video camera attached. The laparoscope projects a magnified view of the Fallopian tubes onto a monitor, enabling the surgeon to guide other instruments that are inserted through a small incision just above the pubic hairline. Once the Fallopian tubes are clipped or sealed, the incisions are closed with self-dissolving sutures.
The procedure is usually performed under general anesthesia and takes about 30 minutes. Afterwards, there may be menstrual-type cramping and/or vaginal discharge or slight bleeding. Patients are advised to rest for a day after surgery and to avoid strenuous activity for several days. Complications are rare, but can include infection, bleeding or injury to other organs. Once a woman has healed from the surgery, she should not experience any effects on hormonal production, menstrual cycle, sexual desire or sexual performance. Tubal ligation is very effective but failures can occur. If it does fail, the pregnancy is likely to be a tubal or ectopic pregnancy, which must be surgically removed.
Tubal ligation should be regarded as a permanent form of birth control and undertaken only when a women is quite sure she does not want to bear children. Surgical reversal has been attempted, but these procedures are frequently unsuccessful, always expensive and are not covered by health insurance. Even when a tubal reversal procedure is successful, the formation of scar tissue increases the risk of ectopic pregnancy.
Vaginal sterilization involves approaching the Fallopian tubes through a small incision in the vagina, then clipping or cauterizing them. This method is not often used because the laparoscopic approach provides better visibility of the Fallopian tubes.
Hysteroscopic sterilization is a relatively new, nonsurgical technique that provides permanent tubal blockage and can be performed in a doctor’s office under local anesthesia. A hysteroscope is passed through the cervix, vagina and uterus to access the Fallopian tubes, and a small device is placed into the opening of each tube. After about three months, scar tissue grows around the implanted devices and effectively blocks the tubes. Because the tubes are not completely blocked until this tissue has grown, other contraceptive methods must be used in the interim. A follow-up visit to the doctor is needed to confirm by x-ray that the Fallopian tubes have been successfully blocked. As of 2015, the FDA has also approved an alternative means of verification for hysteroscopic sterilization that uses a transvaginal ultrasound in place of the x-ray to verify proper placement.
This method has been shown to have a high success rate. Side effects reported during clinical trials included mild to moderate pain during the procedure and some vaginal bleeding for a day or so afterwards.
References
1. Hecht, BK. Birth control: surgical sterilization. www.medicinenet.com/surgical_sterilization.article.htm
2. Sexual health: your guide to birth control: surgical sterilization. www.webmd.com/sex/birth-control/birth-control-sterilization
3. Parker WH. A Gynecologist’s Second Opinion. 2003; A Plume Book; Published by the Penguin Group, New York, NY.
4. Mayo Clinic Staff. Birth control: sterilization. www.mayoclinic.com/health/birth-control
5. Stovall TC, Mann WJ Jr. Surgical sterilization of women. http://patients.uptodate.com/topic.asp?file=wom_issu/6214